When a Child Can’t Perform in Spirometry: GINA 2026 Notes: Oscillometry Alternative.
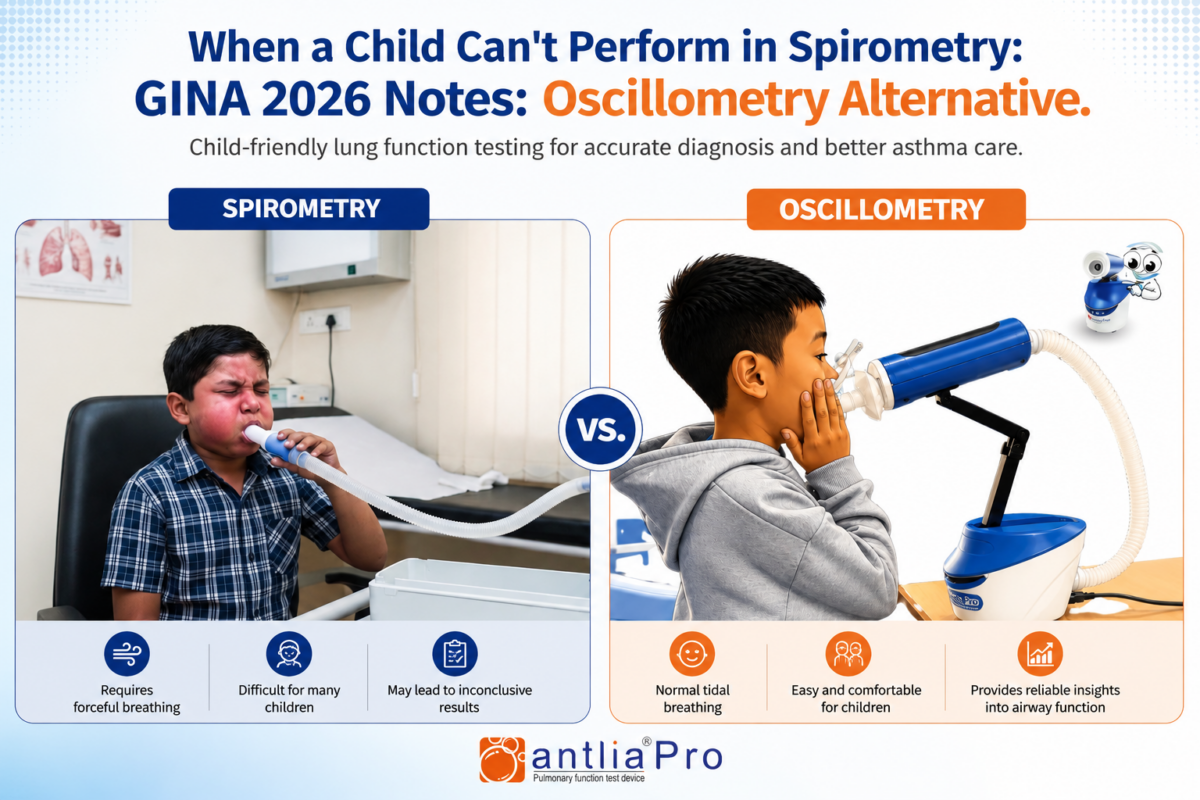
Imagine asking a three-year-old to “breathe in as hard as you can and blow out as fast as possible.” Most clinicians have tried and most have smiled at the result. Traditional spirometry, the workhorse of adult pulmonary diagnostics, demands effort, cooperation, and a degree of respiratory muscle control that young children simply haven’t developed yet. For decades, this left a frustrating gap in paediatric respiratory care: the children who needed lung function assessment the most were precisely those least able to provide it.
Oscillometry quietly changed that equation. And in 2026, the Global Initiative for Asthma (GINA) is paying closer attention than ever.
What Is Oscillometry & Why Does It Matter for Children?
Oscillometry, specifically the Forced Oscillation Technique (FOT), works on an elegantly different principle from spirometry. Rather than demanding a forced expiratory manoeuvre, it superimposes small-amplitude pressure oscillations and sound waves, essentially, onto a child’s normal tidal breathing. The respiratory system’s response to these oscillations reveals its mechanical properties: resistance (how much the airways impede airflow) and reactance (a measure of the elastic and inertive properties of the lung tissues and airways).
The practical implication is profound: a child simply needs to breathe normally, mouth sealed around the mouthpiece, for 30–45 seconds. No coaching for a “big blow.” No repeated failed attempts that frustrate child and technician alike. No risk of fainting from a Valsalva maneuver.
The GINA 2026 Strategy Report explicitly recognises this advantage, noting that oscillometry is “a non-invasive effort-independent lung function test obtained during quiet tidal breathing, which can be performed in children as young as 3 years.” This is not a minor footnote; it represents a paradigm shift in how early-life lung disease can be objectively characterised.
The Diagnostic Gap in Young Children: Where GINA Highlights the Need
According to GINA 2026, asthma is the most common chronic disease of childhood, accounting for a significant proportion of school absences, emergency department visits, and hospitalisations. Critically, symptoms frequently commence during the early childhood years, yet the very tools used to confirm asthma (spirometry, bronchial provocation testing) are described in the report as having “no major role in the diagnosis of asthma” in children aged five years and younger, precisely because most cannot perform reproducible expiratory manoeuvres.
This leaves clinicians in a diagnostically uncomfortable position. A preschooler presenting with recurrent wheezing, nocturnal cough, and exercise-related breathlessness fits an asthma phenotype clinically, but without objective lung function data, confirming the diagnosis and quantifying airflow limitation is largely dependent on treatment response and clinical judgment.
Oscillometry addresses this gap directly. The GINA 2026 report notes that alternative lung function measures, including oscillometry, “are available for children as young as 3 years old” and can be used to “assess bronchodilator responsiveness.” In the context of suspected asthma in a young child, the ability to demonstrate objective bronchodilator reversibility using a non-invasive, effort-independent technique is clinically transformative. It provides the kind of physiological evidence that strengthens or appropriately challenges a working diagnosis.
What Oscillometry Actually Measures: A Clinical Perspective
In paediatric practice, the key oscillometry parameters clinicians rely on are:
Respiratory Resistance (R5, R20): Measured at 5 Hz and 20 Hz oscillation frequencies respectively. R5 reflects total (central + peripheral) airway resistance, while R20 captures predominantly central airway resistance. An elevated R5 with a relatively preserved R20 suggests peripheral or small airway disease — a finding that spirometry may miss entirely.
Respiratory Reactance (X5): Reactance at 5 Hz is perhaps the most sensitive oscillometry marker in paediatric asthma. In healthy children, X5 is near zero or slightly negative. In the presence of peripheral airway obstruction, X5 becomes markedly negative, reflecting reduced lung compliance and air-trapping that conventional spirometry does not detect.
Resonant Frequency (Fres): This is the frequency at which reactance crosses zero. In obstruction, Fres shifts to a higher frequency, indicating mechanical stiffening of the respiratory system.
Area of Reactance (AX): An integrated measure of reactance between 5 Hz and Fres, AX provides a composite marker of small airway dysfunction and has shown strong sensitivity to bronchodilator-induced change in paediatric studies.
Together, these parameters allow clinicians to characterise not just whether obstruction is present, but where in the airway tree it is localised, a distinction with therapeutic implications.
Oscillometry and the GINA Framework: Practical Application
GINA 2026 positions oscillometry within a tiered diagnostic framework. For children aged five and under, it is recommended “when feasible and accessible” to document responsiveness of airflow limitation or airway hyperreactivity. The report is candid about current limitations, acknowledging “a lack of standardized reference values” an important caveat that clinicians must bear in mind when interpreting results.
This is not a limitation of the technology; it is a limitation of where the evidence base currently stands. Oscillometry measurements differ between devices, and GINA 2026 specifically advises that “device-specific reference values should be used.” For clinical practice, this means selecting equipment from manufacturers who provide validated paediatric reference data and understanding that results are not interchangeable across platforms.
For children aged six and older who can attempt but struggle with reliable spirometry, oscillometry serves a complementary role. It can confirm airflow limitation when spirometry quality is poor, detect peripheral airway obstruction invisible to FEV1, and provide a more sensitive endpoint for monitoring treatment response. This aligns with GINA’s broader goal of objectively quantifying lung function to guide personalised management.
From Research to the Clinic: Why Now Is the Moment
The referenced key study cited in GINA 2026 (Ducharme FM, Chan R., Annals of Allergy, Asthma & Immunology, 2025) synthesizes the diagnostic, assessment, and monitoring roles of oscillometry across the paediatric and adult spectrum signalling that the technique has graduated from research tool to clinically actionable test.
For pulmonologists, paediatricians, and respiratory care teams working with young patients, the clinical case for oscillometry is now supported by international guideline recognition. The remaining barriers equipment cost, operator training, and lack of universal reference standards are now being navigated toward resolution as the technology matures.
GINA 2026 reflects the field’s growing consensus: oscillometry is not a second-best substitute for spirometry. It is a fundamentally different tool, uniquely suited to the youngest and most vulnerable patients in our clinics, and increasingly essential to the complete assessment of paediatric lung function.
References: GINA Strategy Report 2026 (Global Initiative for Asthma); Ducharme FM, Chan R. Oscillometry in the diagnosis, assessment, and monitoring of asthma in children and adults. Ann Allergy Asthma Immunol 2025; 134: 135–143.
This article is intended for healthcare professionals and is for informational purposes only. Clinical decisions should be based on individual patient assessment and current guidelines.